The pandemic forced researchers to reassess our current understanding of lung and respiratory biology, which highlighted a neuropeptide better known for its role in migraines. Calcitonin gene-related peptide (CGRP) is abundant in the airways and is secreted mainly by sensory nerve fibers, as well as a rare population of bronchial epithelial cells called pulmonary neuroendocrine cells (PNECs). CGRP functions include vasodilation, inflammation modulation, and tissue repair. Whether CGRP had any direct relationship with SARS-CoV-2 infection was an open question. A 2024 study published in the Journal of Virology answered that question, and the answer is not what many might have expected (1).
CGRP Rises in Critical COVID-19 Cases, and Tracks with the Virus
The team first focused on the analysis of patient samples. Using an enzyme immunoassay (EIA), they measured CGRP in plasma from cohorts covering healthy controls, non-COVID-19 patients, and COVID-19 patients stratified by severity (mild/moderate, severe, and critical). Critical patients showed elevated CGRP levels compared to all other groups (P=0.0194 vs. healthy controls; P=0.0044 vs. severe COVID-19), while levels in mild/moderate and severe cases did not differ from controls.
Since plasma reflects spillover from tissue, the team directly analyzed the lung. They measured CGRP in bronchoalveolar lavage (BAL) samples from critical COVID-19 patients, normalized to total BAL protein. Among patients who were SARS-CoV-2-positive in their BAL – representing early active viral replication – CGRP was elevated compared to non-COVID-19 controls (P=0.0121), and levels correlated positively with viral RNA copies in those same samples (P=0.0010; R2=0.998). In patients whose BAL was SARS-CoV-2-negative, which represented a later stage after viral clearance, CGRP had returned to baseline levels. Therefore, the neuropeptide appeared to rise with the virus and fall once it was cleared.
CGRP Directly Inhibits SARS-CoV-2 Infection in Bronchial Cells
While the correlation in patient samples is suggestive, it cannot be used to establish causation. Therefore, the team shifted their analysis to a controlled in vitro system. They used Calu-3 bronchial epithelial cells – a well-characterized model permissive to multiple SARS-CoV-2 variants – and tested whether CGRP or its metabolically stable analogue serinyl-CGRP2–37-amide (SAX) could directly block infection.
Pre-treating Calu-3 cells with CGRP or SAX for 24 hours before viral exposure inhibited infection with both the Omicron and Alpha variants of the virus in a dose-dependent manner. At 10-6 M CGRP, relative SARS-CoV-2 RNA in culture supernatants dropped to 0.61± 0.08-fold compared to 1.0 ± 0.13-fold in untreated cells (P=0.0432). Viral titers measured with a 50% tissue culture infectious doses (TCID50) assay trended in the same direction (P=0.0761). The inhibitory effect was not limited to pre-treatment: post-infection addition of CGRP or SAX, maintained throughout a four-day culture period, suppressed infection to a similar maximum extent. Therefore, the virus could be blocked both before and after it made initial contact with cells.
CGRP Receptor Signaling Is Essential for Antiviral Activity via Modulation of Viral Entry Pathways
To resolve the mechanism of the CGRP-mediated block of SARS-CoV-2 infection, the team asked whether the inhibition required the cognate CGRP receptor – a heteromeric complex composed of the calcitonin receptor-like receptor (CLR, also known as CALCRL) and the receptor activity-modifying protein 1 (RAMP1). Flow cytometry confirmed that approximately 10% of Calu-3 cells co-expressed CLR and RAMP1 at the cell surface. Pre-treatment with the CGRP receptor antagonist BIBN4096 had no effect on baseline infection, but completely abolished CGRP-mediated inhibition of both Omicron and Alpha variants. This suggested that the anti-viral activity was receptor-dependent.
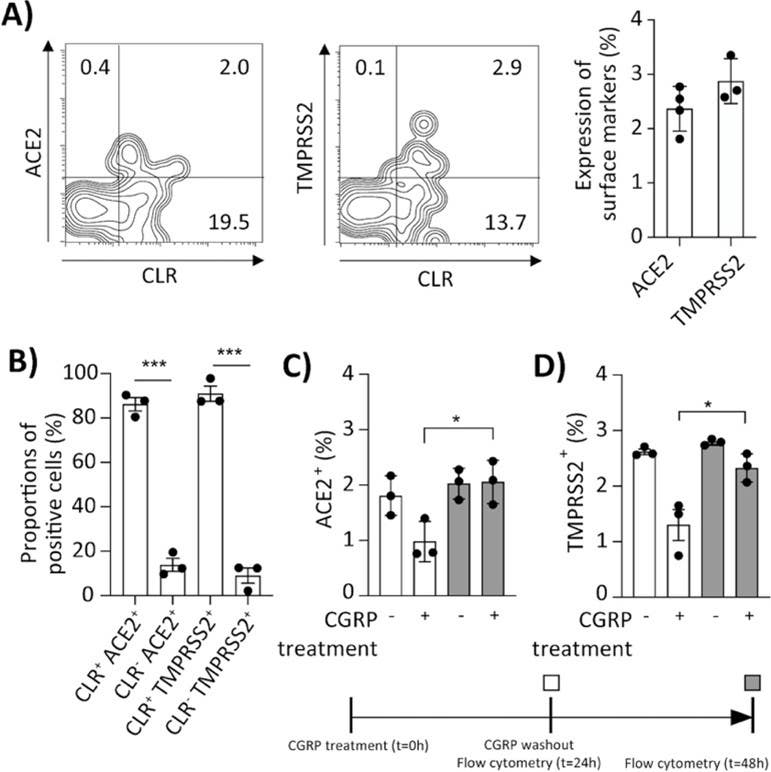
Figure 1. CGRP decreases ACE2 and TMPRSS2 surface expression in Calu-3 cells. (A and B) Representative flow cytometry contour plots showing surface expression of CLR and either ACE2 or TMPRSS2 in untreated Calu-3 cells. In (A), the graph shows the mean ± SEM (n=3–4 independent experiments) percentages of ACE2 or TMPRSS2 positive cells. In (B), the graph shows the mean ± SEM (n=3 independent experiments) proportions of CLR/ACE2 or CLR/TMPRSS2 double-positive vs. single-positive cells expressing ACE2 or TMPRSS2 but not CLR. (C and D) Calu-3 cells were left untreated or treated for 24 h at 37°C with 10−6M CGRP, followed by washout of CGRP and further incubation for 24 h. Surface expression of ACE2 or TMPRSS2 was determined immediately after CGRP treatment (white bars) or the next day following CGRP washout (gray bars). Graphs represent mean ± SEM (n = 3 independent experiments) percentages of positive cells. In all graphs, the statistical significance was evaluated by the Student’s t-test.
Image taken from Bomfim et al. (2024). https://doi.org/10.1128/jvi.00128-24.
To characterize CLR surface expression, the researchers used Alomone’s Anti-CRLR/CALCRL (extracellular)-FITC Antibody (#ACR-060-F) (Figure 1), which was designed for live-cell flow cytometry and targets an extracellular epitope of CLR. This enabled accurate surface staining without fixation artifacts – a useful distinction when mapping co-expression relationships between a signaling receptor and viral entry molecules on the same cell.
Those entry molecules were exactly what CGRP was targeting. Flow cytometry showed that ACE2 and TMPRSS2 – the two primary SARS-CoV-2 entry receptors – were almost exclusively expressed on CLR-positive Calu-3 cells. Following 24 hours of CGRP treatment at 10-6 M, surface expression of both ACE2 and TMPRSS2 dropped by approximately half. When CGRP was washed out and cells were cultured for an additional 24 hours, expression of both receptors recovered to baseline levels. The effect was reversible and tightly linked to receptor activation. The mechanism pathway is: CGRP → CGRP receptor activation → ACE2/TMPRSS2 downregulation → reduced viral entry.
A Connection to Drugs Already in Clinical use
This mechanism becomes more clinically interesting in light of the drugs that already target this receptor. Several FDA-approved therapies for migraines act directly on this pathway: Erenumab (Aimovig) is a monoclonal antibody that targets the CLR/RAMP1 receptor complex itself, and Fremanezumab, Galcanezumab, and Eptinezumab bind CGRP directly. Small-molecule receptor antagonists – including Ubrogepant and Rimegepant – block signaling at the receptor level.
These drugs have been prescribed to millions of migraine patients, in whom CGRP-mediated trigeminovascular signaling drives the pathology. The same receptor that drives migraine pain in the trigeminal system appears to mediate anti-viral protection in the lung. Blocking it in one context is the goal – blocking it in the other could, in principle, remove a natural brake on pulmonary SARS-CoV-2 replication.
The study authors note that two published cohort studies found no increased COVID-19 risk or worse outcomes in migraine patients on CGRP-targeting therapies (2, 3). They interpret this as consistent with their findings: those cohorts were younger and non-critical, and therefore comprise groups in which CGRP levels would not be expected to be elevated anyway. The concern, they argue, applies specifically to elderly patients with early critical COVID-19 – exactly the group where pulmonary CGRP appears to be providing protection against COVID-19.
Rather than avoid CGRP-targeting drugs for migraine treatment, this implies that receptor biology in disease-specific contexts should be carefully considered. The same molecular target can have opposite functional consequences depending on tissue, cell type, and disease stage. While not a complication unique to CGRP, this is a good example of why pathway-level understanding matters more than target-level assumptions.
Neuroimmune Signaling in Viral Infection
The study has uncovered some genuine insights, but it’s important to acknowledge its limitations. The BAL cohort is small (n=4 per group), and the Calu-3 model, while useful, doesn’t fully recapitulate the complexity of the infected lung. Moreover, the causality between rising CGRP and viral clearance in patients cannot be formally established from correlational data alone. The source of elevated pulmonary CGRP during infection also remains partially unresolved, though early research implicated direct activation of lung-innervating sensory nerves by the SARS-CoV-2 papain-like protease (4).
What the data do establish is a receptor-dependent, reversible mechanism by which a pulmonary neuropeptide suppresses the surface expression of viral entry receptors on bronchial epithelial cells. This effect correlated with the timing of viral clearance in the most severely ill patients. For those working at the intersection of neuroimmunology and respiratory infection, or developing CGRP receptor-targeted therapies, both the finding and the caution it implies are worth following.
 Antibody")
-FITC Antibody")
 Antibody")